When I think about the coronavirus pandemic, I try to think of it from two different viewpoints at once: what is the risk to myself and my family, and what is the risk to my broader community? The first viewpoint allows me to get the right ‘anxiety setting’ on my personal stress dial. We generally think of anxiety as something to be avoided, but anxiety is ‘adaptive’ – it exists for a reason, to make us more aware of impending danger, more ready to take action if needed. Anxiety becomes a problem when it isn’t scaled to the actual level of threat, and when it doesn’t lead to actions which reduce threat. I like to know as much as I can about what ‘threat level’ SARS-CoV-2 poses for me and my family so I can gauge whether my anxiety dial is set too high… or too low. If I happen to be in a group that is not especially threatened by SARS-CoV-2, my personal anxiety might be relatively low (whew!). The truth is, many of us can be fairly confident that we could survive a SARS-CoV-2 infection, possibly without ever knowing we were infected. I hope that the data I show below helps reduce personal anxiety for a number of those reading this post.
BUT if we relax our vigilance because we are feeling less anxious, we will raise the overall risk to our communities. Humans are social beings, and we are all members of a number of different communities: our families, our friend circles, our schools, churches, towns, neighborhoods, our states, our countries, and our global community. Community risk is different from personal risk because even if we happen to be in a low risk group, our communities included people who are in high risk groups. We must always be aware that our actions directly impact their risk level, anxiety, and health. And because communities are made up of many people, we must think about risk in terms of populations rather than just individuals. Even if every individual in a large community had a relatively low risk of fatality, say 0.2% (1 out of 500) from a coronavirus infection, if that community included 5,000 people, that would mean about 10 members of the community would die if all community members became infected. If ‘community’ means a city of 500,000 people, like Tucson or Kansas City, then 1,000 people would die. Maybe that number seems small or unpersonal, until we picture the 1,000 funerals that wouldn’t happen if we as a community could keep infection rates low. In a city of around 10 million (like Los Angeles, Paris, Bangkok), that would mean 20,000 ‘extra’ funerals, or 55 a day, every day, for a year.
I hope with this post that I manage to lower personal anxiety for many of you, while reinforcing that, regardless of personal risk levels, we all must remain vigilant and persistent in our fight to block the spread of SARS-CoV-2 through our communities. Until we have a vaccine, the only tools we have available to us to stop the spread of this infection are mask-wearing, social distancing, and absolutely avoiding ‘high spread’ conditions. Those tools are practical and not political, regardless of how they are discussed by politicians, news media, or social media, and they work, but only if used by all of us as a community.
Will I get infected?
Obviously this depends both on the infection rates in your community and your own activities within that community. If infection rates in your community are low, then you are at low risk of infection even if you are less careful about social distancing and mask wearing. Of course, infection can spread quickly if community members are engaging in ‘high-spread’ activities. Mask wearing and social distancing reduce the chances of becoming infected across the board, but if community infection levels are high, even those that social distance and wear masks can become infected. For more, see my previous post about ‘super-spreader’ events and also link to the National Geographic interactive.
Does my age affect how likely I am to become infected?
Age and risk behavior are obviously correlated when it comes to how people respond to this pandemic. We are seeing many more news stories about pool parties with 20-somethings than with senior citizens. At the same time, those under 20 are much more likely to have asymptomatic infections than those over 60. Generally, though, it looks like, if exposed to SARS-CoV-2, we are all equally likely to become infected. The chart below, from the Massachusetts coronavirus ‘dashboard’, shows the number of Massachusetts residents by age out of 100,000 that have had a positive SARS-CoV-2 test. For scale, if these were shown as percentages, the highest number (5,335) would be 5%. The proportion of people testing positive is roughly the same for people between the ages of 20 and 79, suggesting that adults in this age range are catching this virus at about the same rate.
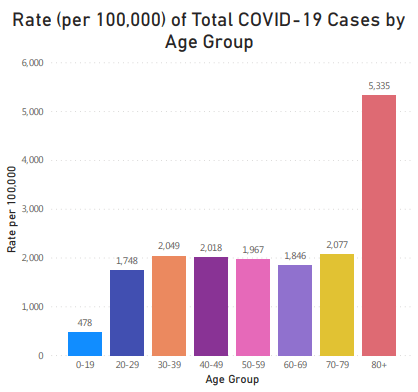
What about those under 20 and over 80? The numbers shown here reflect both the infection rate AND the testing rate. If a person is infected but not tested, they will not show up in these numbers. Because those under 20 generally do not experience bad symptoms from this infection, and because the coronavirus test is unpleasant and not necessarily easy to get, infections in the youngest age group are undercounted. The high numbers for the 80+ age range are also a reflection of infection rate and testing. Being in a care facility increases the chance of being exposed to the virus and of becoming infected. Senior adults also have a high rate of testing because they are in a known risk category and are often in care facilities where testing is done weekly. Generally speaking, though, most of us are probably equally likely to get infected with this virus, if we are exposed.
If I am infected, will I show symptoms?
In my house we have three adults and two kids. The two kids and I caught this recent cold, but the other two adults did not. Did the virus ‘miss’ them somehow? Very unlikely, given that we all share the same space with each other, and the three of us with this cold were sneezing up a storm. All five of us were probably infected, but only three experienced symptoms, so we say the two without symptoms did not ‘catch’ the disease.
The word “disease” specifically refers to disfunction in our own bodies no caused by an injury. Not all infections cause disease, and not all diseases are caused by infection. Saying someone has COVID-19 is different from saying someone is infected with this coronavirus (SARS-CoV-2). COVID names the disease, SARS-CoV-2 names the virus that can cause COVID disease. While everyone in my house was probably infected with a ‘cold’ virus, only three of us showed ‘disease symptoms’. Likewise, not everyone who is infected with SARS-CoV-2 shows COVID-19 symptoms. In fact, the CDC currently estimates 40% of those infected with SARS-CoV-2 are asymptomatic and never experience obvious COVID-19 symptoms. Most young people have asymptomatic infections (80% or more), and while the percent of asymptomatic infections decreases with age, even as many as 30% of those 70 or older can be infected and not show symptoms. In fact a recent study from a Chicago nursing home found that 37% of residents who tested positive for coronavirus never showed symptoms.
Why are some people asymptomatic, but others get really sick?
Why did two people in my house of five escape without obvious cold symptoms? Why do only around 60% of SARS-CoV-2 infections cause COVID symptoms? Why are young people most often asymptomatic?
Whether we experience symptoms as a result of an infection depends on many different aspects of the relationship between that pathogen and our own immune system. How many individual viruses were we exposed to? How well did each of those viruses manage to attach to and get into our cells? How fast were new viruses produced and released? When did our immune system recognize there was a problem? How fast did our immune system respond, and how well? Did our immune response clear virus without causing excessive damage to our own bodies?
We are each born with a genetic ‘toolbox’ that our immune systems can pull from. Some of these tools are nearly identical from person to person (our ‘innate immunity’), some tools vary a lot between people (our HLA molecules), and some tools we each make from scratch, every one of them unique (B-cells/antibodies, T-cells), but which we can save if they worked well (B and T memory cells). Our immune system toolbox in any one moment of our lives includes the tools that it came with and ones that we’ve made in response to previous infections and vaccinations. In addition, we can also make new tools to respond to brand new challenges, but this takes times (7-10 days after infection). Because we build up our tool collection over time, children have fewer of the ‘made from scratch’ tools than adults. But having a disorganized or faulty toolbox may make tools hard to find, or easy to lose tools. Age, nutrition, stress, disease and genetics all affect how ‘strong’ our toolbox is, and over time we all eventually begin to lose some of our immune ‘toolset’. While our immune system can usually ‘make do’ with the tools it still has, the result is often not quite as good.
Why are so many people asymptomatic when infected with SARS-CoV-2? A number of factors are probably at play. If a viral infection is slow to start, our immune systems have more time in which to respond before the infection begins to cause damage. Reducing infection numbers can limit the amount of exposure any one of us has to this virus. If we reduce the numbers of people who can spread the virus, we reduce the chances that we are exposed, and also the amount of virus we are exposed to, if exposed. Masks filter out particles from the air before we breathe it in. Even if a mask is not 100% effective, they can still reduce the number of viral particles we are exposed to, slowing the beginning of the infection process. Immune memory may also be involved. A number of coronaviruses are known to cause ‘the common cold’. It is possible that some of us have immune memory cells developed in response to infections by those other coronaviruses that can also be useful against SARS-CoV-2. Vaccines for some other viruses may also be able to produce immune memory that allows some ‘coverage’ for SARS-CoV-2. (See this WP article for more information and sources). If a person has memory cells for other infections that have some ability to recognize SARS-CoV, they might be able to mount a partial immune response even early in the infection. This response may not be enough to clear the virus before it causes symptoms, but it may reduce the severity and length of symptoms.
Why are symptoms so much worse for some people?
Why did I get this cold, but not the two other adults in my house? I know from experience that there is a type of cold that I get over and over again. When I was a kid, I would get a head cold that eventually turned into croup. As an adult, the cold feels exactly the same, but ends with me getting laryngitis. I tend to get this cold every February… and this year, again in August. My immune system toolbox is missing the perfect tools to fight this particular kind of virus and has to make do with a set of tools which are not quite right, but eventually get the job done Each of us has some weaknesses in our immune response – we don’t recognize every possible pathogen equally well.
Having this genetic variation is actually an adaptive advantage for our population: while some of us may be susceptible to specific pathogens, it is very difficult for any one pathogen to evade all of our different immune responses. On the plus side, we survive as a species. On the minus side, some fraction of us are more prone to infection and death from any given pathogen. In the case of coronavirus pandemic, this means that some fraction of our population, across all age ranges, is going to have a more difficult time with this infection that other people, and because this weakness is due to the specific nature of a person’s immune system, we can’t know in advance exactly who these people will be. We can, however, tell that this number is fairly low because COVID severity and fatality rates depend mostly on age and health.
More about age and health risks in Part 3
